Thanks Eugene, for inviting me to join the conspiracy -- and thanks to those who welcomed me in advance of my actually doing anything to deserve such treatment. To be sure, as a former employee of the Federal Trade Commission, the whole conspiracy thing is a bit disconcerting. Thankfully, this particular conspiracy is to promote (rather than restrain) trade -- this time, of ideas.
Yesterday's Wall Street Journal had an op-ed on the virtues of caps on non-economic damages in medical malpractice cases. Non-econ caps are ground zero in the debate over medical malpractice reform.
To proponents, non-econ caps are a silver bullet, simultaneously targeting frivolous lawsuits, excessive damage awards, run-away juries, and high medical malpractice premiums. To critics, non-econ caps are both ineffective (since they will not lower malpractice premiums or the cost of health insurance coverage) and unfair (since they reduce damage awards to the most severely injured, and disproportionately affect women, children, and the elderly).
I've spent the past few years doing a series of empirical papers on medical malpractice, with several co-authors from the University of Texas (Charlie Silver, Bernie Black, and Bill Sage), and Georgetown (Kathy Zeiler), including a forthcoming paper in the Journal of Legal Analysis estimating the impact of such caps. So, I thought I'd join the Conspiracy by highlighting some of our findings, in this and other works, which call into question/complicate some of the claims in the WSJ editorial.
Today, I'll provide general background on damages caps. Tomorrow, I'll address the impact of damages caps on verdicts and payouts in tried cases, and payouts in settled cases. After that, I'll address the issue of damages caps and access to medical services. Finally, I'll turn to the larger social policy issues raised by damages caps.
Let me start with some general background. In malpractice cases, one can recover two types of compensatory damages: economic, and non-economic. Economic damages are things like lost wages and medical expenses. Non-economic damages are less concrete, and include things like pain and suffering, loss of enjoyment of life, loss of consortium, and the like.
Non-economic damages have been a frequent target of tort reformers, beginning with the successful campaign to adopt a cap on such damages as part of the Medical Injury Compensation Reform Act ("MICRA") enacted by California in 1975. Over the intervening years, campaigns have been fought to enact damages caps in numerous states. The campaign to enact such caps is usually triggered by a malpractice "crisis," marked by sudden and dramatic increase in malpractice premiums.
Several states have enacted non-econ caps only to see them struck down by the state Supreme Court. This is what happened in Illinois twice in the past several decades, and we are waiting to see whether it will happen again — although I wouldn't bet on it this time around.
Although it is common to speak of non-econ caps as a unitary entity, they actually come in numerous varieties, reflecting the design choices of each individual state legislature. Consider a couple of the moving parts:
What should the dollar level of the cap be set at?
Should the dollar level of the cap be indexed for inflation?
Should the cap vary by the number and type of defendants? For example, should doctors have a lower cap than hospitals? What about a case in which there are both types of defendants? Should separate caps apply to each?
Should the cap cover non-economic damages, total damages, or both?
Should there be a separate cap on punitive damages (which are rare in malpractice cases against doctors and hospitals, but less so in cases against nursing homes)?
Should the cap only cover medical malpractice, or should it apply more broadly?
Should cases in which the plaintiff is deceased have a different cap level than those in which the plaintiff is not?
At present, 31 states have caps on non-economic damages or total damages or both. (I exclude caps on punitive damages to keep things simpler). The Table below provides a brief summary of the cap that is in effect in each state, sorted by cap type and level.
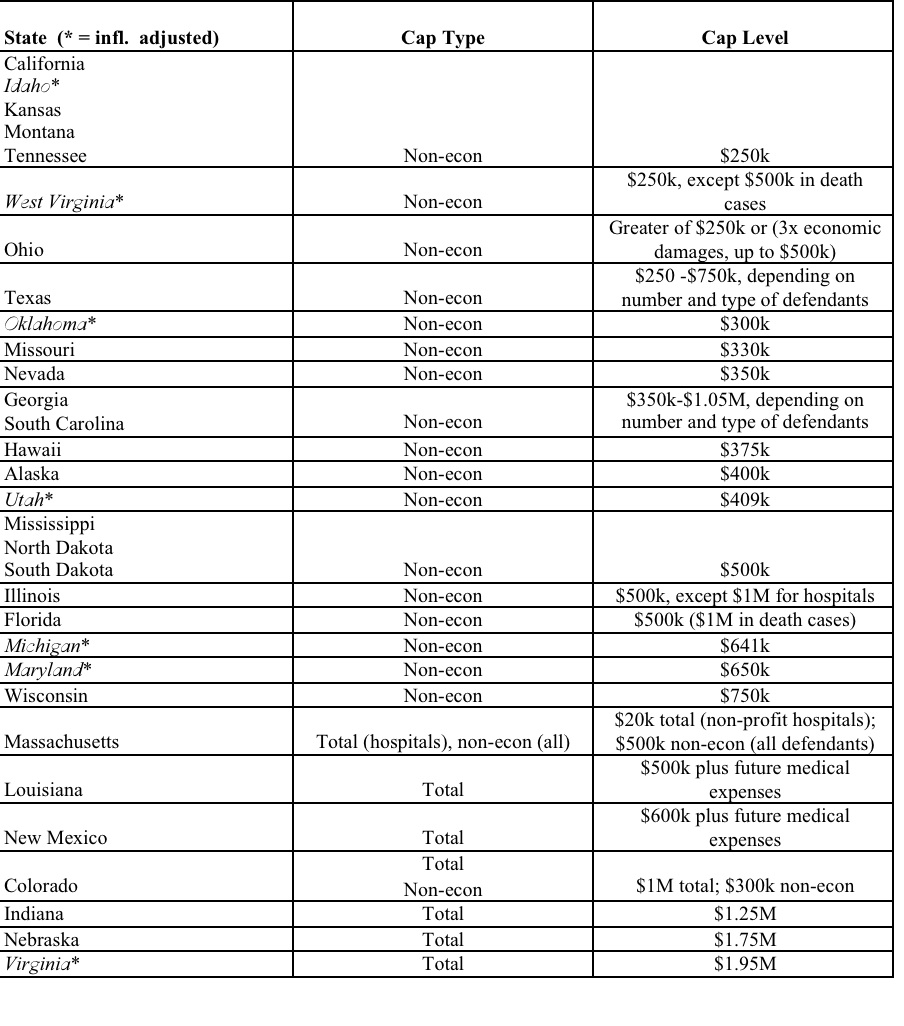
Thus, there are 24 different variations among the 31 states that have adopted a damages cap. The most popular cap is the flat $250,000 cap chosen by California, and since copied by four other states. Those looking for a deep principle of justice explaining the logic of this cap level should prepare themselves for disappointment: as this first-rate student note carefully documents, the level of the California cap was quite arbitrary. As part of her research, the author emailed the principal legislative sponsor, and asked him why they settled on $250,000, and received the following response:
The theory was that you could never really and adequately compensate for pain and suffering, no matter how much money you provided. Money just doesn't do it. But $250,000 (in addition to meeting the medical and other needs of the patient), properly invested to the extent that it elevated the quality of life over and above the post-injury status, was thought to be enough to do that job.
That's enough for my first-ever blog posting. Tomorrow, I'll address how damages caps affect payouts, including their interaction with plaintiff demographics.
Related Posts (on one page):
- Damage Caps and Medical Malpractice VII
- Damage Caps and Medical Malpractice Litigation: VI
- Damage Caps and Medical Malpractice Litigation: V
- Damage Caps and Medical Malpractice Litigation: IV
- Damage Caps and Medical Malpractice Litigation: III
- Damage Caps and Medical Malpractice Litigation: II
- Damage Caps and Medical Malpractice Litigation