In Madness and Civilization, Michel Foucault documented a remarkable continuity of confinement through different stages of Western European history, from the lazar houses for lepers on the outskirts of Medieval cities, to the Ships of Fools navigating down rivers of Renaissance Europe, to the establishment in the seventeenth century of the Hôpital Général in Paris — an enormous house of confinement for the poor, the unemployed, the homeless, the vagabond, the criminal, and the insane.
“Leprosy disappeared,” Foucault writes, “the leper vanished, or almost, from memory; these structures remained. Often, in these same places, the formulas of exclusion would be repeated, strangely similar two or three centuries later. Poor vagabonds, criminals, and “deranged minds” would take the part played by the leper . . . . With an altogether new meaning and in a very different culture, the forms would remain—essentially that major form of a rigorous division which is social exclusion but spiritual reintegration.”
Social exclusion unites the asylum and the prison. The question that I ask in my research is whether we should think of the two populations as somehow linked. Is it possible that today’s category of the “criminally deviant” is tied to yesterday’s category of the “mentally defective”? In our social research, should we think of the two populations as a whole, rather than as two separate parts?
I am by no means suggesting that the same people have been moved from one institution (the asylum) to another (the prison). That is far too simplistic – for at least three important reasons.
Mental Illness: First, although the rate of mental illness among prison inmates is probably higher than among the general population and although the problems surrounding mental illness in jails and prisons have reached crisis proportions, it’s not the case that our prisons today are overwhelmingly housing persons with mental illness. For one thing, the war on drugs has taken an enormous toll on African-American communities, and has contributed to an unconscionable increase in black male incarceration that has nothing to do with mental illness. Bruce Western at Princeton documents this better than anyone in his new book, Punishment and Inequality in America.
Estimates of the number of mentally ill inmates vary. According to a 1999 report by the DOJ, about 283,800 inmates in prisons and jails suffered from mental illness at the time – which represented about 16% of jail and state prison inmates. A more recent 2006 DOJ study reported that 56% of inmates in state prisons and 64% of jail inmates across the country reported mental health problems within the past year. Steven Raphael at Berkeley has a fascinating paper and he finds that deinstitutionalization from 1971 to 1996 resulted in between 48,000 and 148,000 additional state prisoners in 1996, which according to him, accounted “for roughly 28 to 86 percent of prison inmates suffering from mental illness.”
A new paper by Steven Erickson and his colleagues reviews the literature on prison mental illness and shows that the estimates for mental illnesses, broadly defined, range from 16% to 90% and for severe mental illness from 6.4% to 39%. “These rates,” they suggest, “are well above those found in the general population of approximately 30% for mental illness and 6% for severe mental illness.” The paper is extremely skeptical of these estimates and casts doubt on the surveys based on methodological shortcomings.
For sure, it is exceptionally difficult to compare mental hospital residents of the 1950s to prison populations of the 1990s because the definitions, diagnoses, and medical routines have changed so much. Remember, the whole infrastructure of our mental health system has collapsed – making it unrealistic to measure the key attribute of “prior mental health contacts.” Moreover, drug use and psychotropic medications have changed enormously. But despite all that, the two populations must differ along somewhat-objective criteria of mental illness.
Race, Sex and Age: Second, the demographics of the two populations are different, as I discuss here in the Texas Law Review at pages 1781-1784. The prison population today is, overall, younger, much more male, and more African-American than the mental hospital populations at mid-century. In 1966, for example, there were 560,548 first-time admissions to mental hospitals, of which 310,810 (55.4%) were male and 249,738 (or 44.6%) were female. In contrast, new admittees to state and federal prison were consistently 95% male throughout the twentieth century. In 1978, African Americans represented 44% of newly admitted inmates in state prisons. That same year, minorities represented 31.7% of newly admitted patients in mental hospitals.
(But note that those populations were also changing internally. Henry Steadman and John Monahan report in a 1984 study that, in their sample, “the mean age at hospital admission decreased from 39.1 in 1968 to 33.3 by 1978. The percentage of whites among admitted patients also decreased, from 81.7% in 1968 to 68.3% in 1978.” There was a similar shift in the prison admissions data: “the mean age of prison admittees was 29.0 in 1968 and 28.1 in 1978" and the percentage of whites among prison admittees decreased from "from 57.6% in 1968 to 52.3% in 1978").
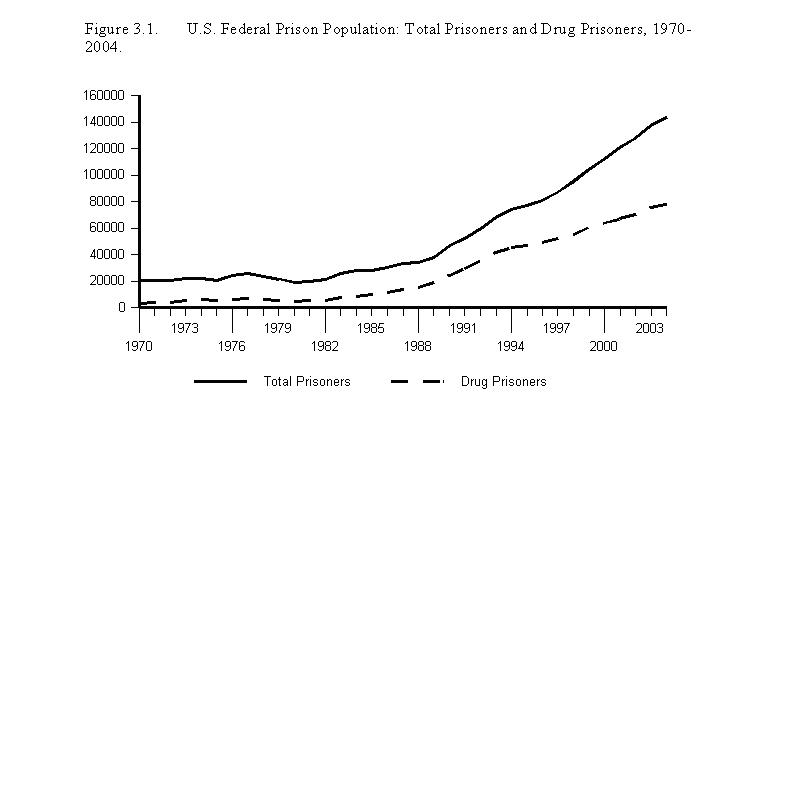
The War on Drugs: Third, a large portion of our current prison population consists of non-violent drug offenders. The war on drugs has helped fill our prison populations, especially our federal prisons. The following graph, from a forthcoming book with Frank Zimring at Berkeley on the Criminal Law and Regulation of Vice, traces the total sentenced population of the federal prison system and the number of federal prisoners for whom the most serious offense was a drug offense:
As I noted before, drug use may intersect in complicated ways with mental health issues, and some users may well be self-medicating. But the numbers associated with the war on drugs clearly transcend these possible connections.
As a result, the story is not simple trans-institutionalization. It is not simply substitution from one institution to another. But that does not mean that the populations are not sufficiently connected or similar in more important ways to be thought of as one – or counted as one. Could it be that we use the categories to socially exclude people we perceive as marginal, disorderly, abnormal? Do we use the categories to sift out those who offend our sensibilities and who we perceive as dangerous? Michel Foucault observed in Madness and Civilization that “There must have formed, silently and doubtless over the course of many years, a social sensibility, common to European culture, . . . that suddenly isolated the category destined to populate the places of confinement. To inhabit the reaches long since abandoned by the lepers, they chose a group that to our eyes is strangely mixed and confused. But what is for us merely an undifferentiated sensibility must have been, for those living in the classical age, a clearly articulated perception.”
Today, the categories of “mental illness” and “criminal deviance” seem very distinct. With the exception of those inmates who are diagnosed as suffering from mental illness, it seems wrong or confused to lump together the insane and the criminal, to mix the two categories. But is it? Will later generations question our own inability to see the continuity of social exclusion and confinement?
One place where the categories seem to be melding together is in the prediction instruments that we use to identify future dangerousness. We are now profiling the criminally dangerous, the mentally instable, and future sexual offenders in very similar ways. I trace the history of our profiling instruments in a new book, Against Prediction: Profiling, Policing, and Punishing in an Actuarial Age.
We’ve seen a rash of new actuarial instruments intended to predict future violent behavior. In terms of sexual violence, these include the Static-99, the Violence Risk Appraisal Guide (VRAG), the Hare Psychopathy Checklist-Revised (PCL-R), the Minnesota Sex Offender Screening Tool (MnSOST-R), the Sex Offender Risk Appraisal Guide (SORAG), the Sexual Violence Risk-20 (SVR-20) and the HCR-20 — as well as, for the very first time, released in 2005, violence risk-assessment software, called the Classification of Violence Risk (COVR).
How accurate are these prediction instruments and how will they affect the profiled populations? John Monahan, a leading authority on prediction instruments, a proponent of these instruments (in fact co-author of the new COVR software), and the director of the MacArthur Violence Risk Assessment project, offers a nuanced assessment. Writing in The Observer, Monahan asks: “How good are psychiatrists and psychologists at distinguishing which people with a mental illness will be violent? Research shows professionals are better than pure chance, but not much. Predicting harmful behaviour is like predicting bad weather. An inaccurate prediction doesn't necessarily mean the clinician or the meteorologist has 'missed something'; it may just mean the science of forecasting has a long way to go.”
Not much better than pure chance. Virginia just adopted a Sexually Violent Predators Act (“SVPA”) in April 2003 that provides for the civil commitment of sex offenders identified based on the Rapid Risk Assessment for Sex Offense Recidivism (RRASOR) – an actuarial instrument. The RRASOR consists of four items (prior sexual offenses, age at release, victim gender, and relationship to victim) and scores as a sum these four items. A score of 4 or more on the RRASOR (the higher scores) is associated with a 5-year sex offense recidivism rate of 37% and a 10-year sex offense recidivism rate of 55%.
Fifty-five percent — and remember, these are persons who have previously been convicted (rightly or wrongly) of a sexually violent offense. That leaves almost half the relevant population misidentified, at least for that 10-year span. Accuracy and inaccuracy may be in the eye of the beholder. (I discuss the reliability of other actuarial instruments in Against Prediction, reviewing studies like these here and here). The question is, how will these new actuarial methods and predictions of future dangerousness shape the people in our total institutions?
UPDATE MAY 4, 2007: John Monahan tells me that Virginia last year changed it's Sexually Violent Predators statute to require not the RRASOR but the Static-99. The Static-99 has slightly different cut-off scores depending on the age of the victim.
Related Posts (on one page):
- Carceral Notebooks, Volume 2: Exploring the Carceral Zone with Nussbaum, Sunstein, Stone, Leitzel, McAdams, and Others.
- Concluding Thoughts on Total Institutions: Future Directions and Critical Reflections.
- Asylums and Prisons: Race, Sex, Age, and Profiling Future Dangerousness.
- Institutionalization vs. Imprisonment: Are There Massive Implications for Existing Research?
- Mental Hospital, Prison, and Homicide Rates: Some More Analyses.
- Mental Hospitalization and Prison Rates in Western Europe:
- On Mental Health Commitments and the Virginia Tech Shooting:
- Bernard Harcourt Guest-Blogging: